Guidance for Medicare Fee-for Service Payment from the Centers for Medicare and Medicaid Services
On Tuesday, March 17, 2020 the Centers for Medicare and Medicaid Services expanded Medicare coverage for telehealth visits, implementing new powers under the coronavirus legislation. These changes temporarily remove originating site and geographic restrictions from coverage of telehealth under Medicare fee-for-service. This coverage applies to all Medicare-approved telehealth services.
On March 30, CMS issued an interim final rule, implementing a large number of blanket waivers and additional changes. These rules went into effect on April 6. We have a separate website detailing them and the 80 newly approved telehealth codes within– CMS COVID-19 Interim Final Rule Summary
On April 30, CMS issued a second interim final rule, implementing significant additional changes for telehealth. Specifically, the rule includes more changes created using the statutory authority of Coronavirus Aid, Relief, and Economic Security Act (CARES Act). These changes come from both new 1135 waivers and the interim final rule. We have a separate website detailing the changes — April CMS COVID-19 Interim Final Rule Summary
- April 7 Dear Clinician Letter
- March 17 Announcement by CMS Administrator Seema Verma
- Press Release
- Fact Sheet
- Frequently Asked Questions (FAQs) – March 17
- Updated FAQs on Medicare FFS Billing – CMS continually updates these (Updated June 19)
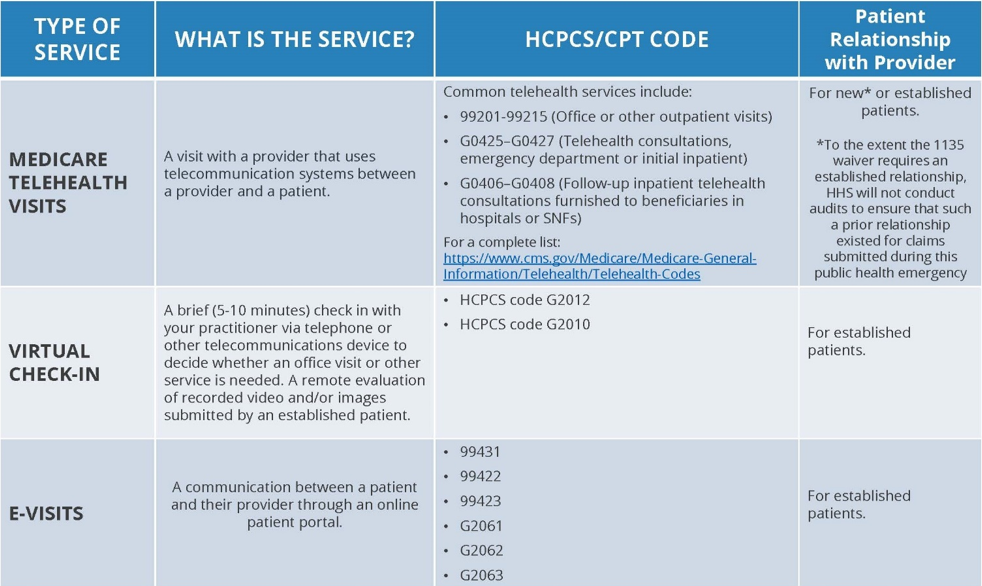
- Infographic
- CMS List of Codes (with audio-only)
{kind=link}
Implementation:
- CMS Implementation Toolkit for General Practitioners
- CMS Toolkit for ESRD Providers
- FFS Telehealth Basics: 2020 MLN Telehealth Services Booklet
- March 27 Nursing Home Telehealth Toolkit
- March 26 FAQ on Enrolling as a Medicare provider under 1135 flexibility
- March 22 Provider Enrollment Relief FAQs
Updated May 8 – In addition to the guidance above, CMS posted an informational video providing answers to common questions about the Medicare telehealth services benefit.
Guidance on the Emergency Medical Treatment and Labor Act
The Emergency Medical Treatment and Labor Act (EMTALA) requires Medicare-participating hospitals and critical access hospitals (CAHs) to:
- Conduct a medical screening exam (MSE)to all individuals who come to the emergency department for examination or treatment for a medical condition to determine whether that individual has an emergency medical condition (EMC).
- Provide necessary stabilizing treatment for individuals with an EMC within the hospital’s capability and capacity.
On March 30, the Centers for Medicare and Medicaid Services revised EMTALA guidance in response to hospitals and CAHs concern with meeting EMTALA compliance due to COVID-19. The revised guidance states that a Qualified Medical Personnel (QMP) may use telehealth to perform the medical screening exam (MSE) without creating an EMTALA liability.
On April 30, CMS issued frequently asked questions (FAQs) clarifying requirements and considerations for hospitals and other providers related to the Emergency Medical Treatment and Labor Act (EMTALA) during the COVID-19 pandemic. The FAQs address questions around patient presentation to the emergency department, EMTALA applicability across facility types, qualified medical professionals, medical screening exams, patient transfer and stabilization, telehealth, and other topics.
- April 30 FAQs for for Hospitals and Critical Access Hospitals regarding EMTALA
- March 30 Revised EMTALA Requirements and Implications Related to COVID-19
Guidance on Medicare Advantage (MA)
Starting in 2020, Medicare Advantage Plans may offer more telehealth benefits than Original Medicare. These benefits can be available in a variety of places, and you can use them at home instead of going to a health care facility.
In response to the coronavirus pandemic, CMS outlined flexibility that Medicare Advantage plans have to help prevent the spread of COVID-19. One emphasis was expanding access to certain telehealth services. CMS clarified the ability to add telehealth benefits to existing plans as well as the flexibility to waive cost-sharing or reduce costs for specific services. Medicare Advantage plans have the flexibility to expand their coverage of telehealth but are not required to expand beyond what is provided in Medicare fee-for-service.
On April 10, CMS released a memo stating that Medicare Advantage organizations and other organizations that submit diagnoses for risk adjusted payment are able to submit diagnoses for risk adjustment that are provided via telehealth visits. In addition, telehealth services can meet the risk adjusted face-to-face requirement when services are provided using interactive audio and video telecommunications system that permits real-time interactive communication.
- April 30 Fact sheet on flexibilities for MA and Part D plans
- April 24 MAO Guidance allowing the provision of smartphones or tablets as a supplemental benefit in order to aid in the use of telehealth or RPM services.
- (UPDATED APRIL 21) CMS Memorandum on MA and Part D
- April 10 Applicability of diagnoses from telehealth services for risk adjustment
- March 10 Press Release