Correcting the Record on Telehealth
March 2024
During the March 12 House Ways and Means Committee Hearing on Expanding Access to Care at Home in Rural and Underserved Communities, a number of already disproven myths about telehealth were publicly repeated. While broader understanding of the benefits and use of telehealth have come a long way, these outdated misconceptions continue to undermine policymaking and must be corrected.
Importantly, the Alliance and its members believe that an in-person visit requirement is never the right guardrail for a telehealth service – because these requirements harm patients with access challenges, such those who are frail or homebound, have transportation issues, or live in rural or underserved areas. Similarly, we believe that a clinician’s time has the same value, no matter if they are supporting a patient virtually or in-person.
Correction #1 – Telehealth Does Not Lead to Increased Fraud
In 2021, the Department of Health and Human Services (HHS) Office of Inspector General (OIG) released a statement clarifying the difference between telehealth fraud and “telefraud”, with the latter involving the use of telemarketing to defraud patients. The letter emphasizes OIG’s investigations, which found that perpetrators billed fraudulently for other items and services, like durable medical equipment or genetic tests, but did not bill for a telehealth visit. Importantly, OIG did not document telehealth services fraud.
In February of 2024, OIG released a report, which found that telehealth services provided to Medicare beneficiaries complied with Medicare requirements and did not show evidence of fraud. The report examined telehealth services provided to Medicare beneficiaries from March 2020 through November 2020, the peak of telehealth usage.
Telehealth is no more susceptible to billing fraud than in-person services. Rather than focusing on telehealth, Congress and the Administration should continue to focus on identifying and addressing fraudulent behavior across the entire Medicare program through tools like a stronger provider enrollment process and enhanced monitoring.
Correction #2 – Telehealth Has Not Been Shown to Drive Overutilization
The Assistant Secretary for Planning and Evaluation (ASPE) has consistently found that the utilization of telehealth among Medicare fee-for-service (FFS) beneficiaries continue to be above pre-pandemic levels, but is not showing signs of growth. As you might expect telehealth service utilization is higher among vulnerable populations due to their greater need for care from the severity and complexity of their illness.
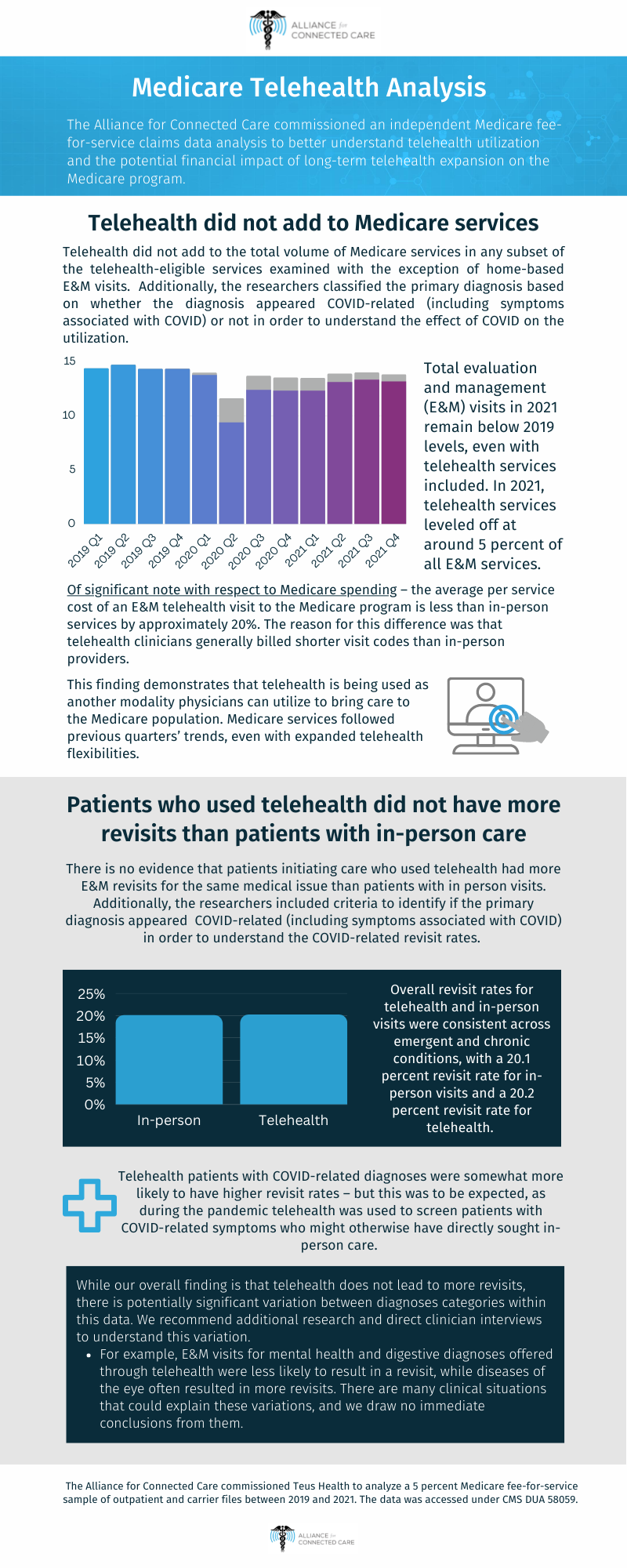
The Alliance and many other organizations have looked telehealth utilization in the context of total Medicare utilization and shown that telehealth services have generally leveled off around 5 percent, while total utilization has not significantly grown. Telehealth did not add to the total volume of Medicare services in nearly all of the telehealth-eligible services examined.
{kind=link}
Robust research has found that telehealth substitutes for in-person care rather than contribute to overutilization. An Agency for Healthcare Research and Quality (AHRQ) funded study, analyzed more than four million primary care encounters, and found little change in health care utilization as telehealth became widely accessed.
The Alliance’s commissioned independent Medicare claims data also found no evidence that patients initiating care who used telehealth had more E&M revisits for the same medical issue than patients with in-person visits.
A study conducted by Epic Research found that follow-up rates were less for telehealth than in-person office visits. Most specialties have greater rates of same-specialty in-person follow-up in the 90 days after in-person office visits than after telehealth visits.
Correction #3 – Telehealth Has Not Been Shown to Increase Spending
A growing body of evidence has found that telehealth is associated with lower no-show and cancellation rates. No-shows cost health care providers $150 billion every year.
An AHRQ-funded study fund that telehealth reduced primary care spending due to lower emergency department utilization and inpatient hospitalizations.
The Alliance’s commissioned independent Medicare claims data also found that the average per service cost of an E&M telehealth visit to the Medicare program is less than in-person services by approximately 20 percent. The reason for this difference was that telehealth clinicians generally billed shorter visit codes than in-person providers.
 Loading...
Loading...